Original article found here.
What Patients Should Know About Cosmetic Surgery and Their Cosmetic Surgeons
Jayne O'Donnell's articles of September 14-15, 2011 entitled "These Women died after having liposuction" and "Cosmetic surgery gets cheaper, faster, scarier: Commoditization opens door to dubious practices" (collectively "Article") jeopardize the safety of your readers considering cosmetic surgery. The Article is filled with false information, and misleads patients regarding how to choose a cosmetic surgeon placing patients at risk.
In order to protect cosmetic surgery patients who read your Article, the American Academy of Cosmetic Surgery ("AACS"), American Board of Cosmetic Surgery ("ABCS"), the Cosmetic Surgery Foundation for Education, Research and Patient Safety ("CSF"), and the cosmetic surgeons who represent the specialty of cosmetic surgery on the American Medical Association ("AMA") House of Delegates, respectfully urge USA Today to correct the false and misleading statements contained in the Article. The authors hereof, and the groups they represent, share the goal of patient safety through education. We were disturbed to learn of the tragedies subject to the Article, and it reminded us why we tirelessly advocate to ensure that only physicians who obtain the necessary education, training, and experience perform cosmetic surgery. Unfortunately, Ms. O'Donnell was misinformed, and the Article relies on anecdotal information rather than peer reviewed articles and fact based evidence.
It is our goal to provide cosmetic surgery patients with valuable and credible information regarding cosmetic surgery, and the education, training, and experience necessary to perform it. To help USA Today correct the misinformation included in the Articles, below is fact-based information regarding cosmetic surgery and who is qualified to perform it:
Plastic Surgery and Cosmetic Surgery Are Not the Same Thing.
Cosmetic surgery and plastic surgery are different specialties requiring different education, training, and experience. Cosmetic surgery involves procedures designed to enhance appearance (Common procedures include breast implants; chemical peels; chin, cheek, and nose augmentation; face lifts; hair transplants; liposuction, and tummy-tucks). Cosmetic surgery was developed, and is practiced, by dermatologists, facial plastic surgeons, general surgeons, gynecologists, oral and maxillofacial surgeons, ophthalmologists, otolaryngologists, plastic surgeons, and doctors from other fields. Unlike cosmetic surgery, plastic surgery is dedicated to reconstruction of facial and body defects due to birth disorders, trauma, burns, and disease.
There are currently no residency programs in the U.S. devoted exclusively to cosmetic surgery. And, residency programs in dermatology, general surgery, obstetrics and gynecology, oral and maxillofacial surgery, ophthalmology, otolaryngology, and plastic surgery do not include training on every cosmetic procedure. Therefore, doctors seeking to learn the vast array of cosmetic surgery procedures must do so after completing their residency training. Understanding this fact is necessary to understanding the difference between "cosmetic surgery" and "plastic surgery."
Residency training required to become board certified in plastic surgery may not include training with respect to many common cosmetic procedures. Therefore, while the title "board certified plastic surgeon" tells you the doctor has received certain training and experience with respect to "plastic surgery," it does not tell you the same thing with respect to "cosmetic surgery," and it does not tell you the doctor has more or less "cosmetic surgery" training than a board certified dermatologist, facial plastic and reconstructive surgeon, general surgeon, gynecologist, oral and maxillofacial surgeon, ophthalmologist, otolaryngologist, or other doctor. Therefore, to find the most qualified doctor for a specific cosmetic procedure, patients must compare doctors' overall (residency and post-residency) training and experience with respect to that procedure.
Cosmetic surgery patients need to understand that the education, training, and experience required for a doctor to become competent in cosmetic surgery is not the same as that required to become competent in plastic surgery. The Article's suggestion to the contrary is simply false. See Diagram A.
Diagram A

Diagram A illustrates the Article's false premises that all board certified plastic surgeons, and only board certified plastic surgeons, are qualified to perform all cosmetic procedures. Cosmetic surgery patients who believe these false premises are misled into relying on incomplete and inaccurate information when choosing their physician. As a result, patients fail to consider many well-qualified cosmetic surgeons, and fail to properly evaluate physicians' education, training, and experience regarding their cosmetic procedure. As a result, their safety is jeopardized by: (1) having their choice of qualified cosmetic surgeons arbitrarily reduced;1 and (2) potentially being directed to physicians with little or no cosmetic surgery experience.
The fact is that there are physicians in various specialties who obtain the necessary post-residency education, experience and training to become qualified to perform cosmetic surgery, and there are others who do not. Therefore, a physician's competence, skill, and ability with respect to a cosmetic surgery procedure depends on their education, training, and experience regarding that procedure, and not on their particular board certification. See Diagram B.
Diagram B
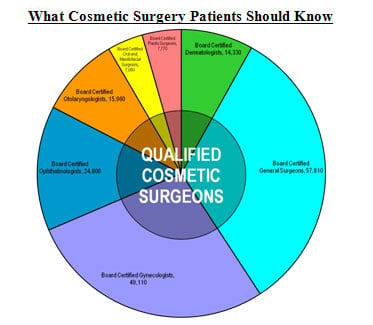
Diagram B correctly illustrates that within each discipline there are physicians who received specialized education, training, and experience in cosmetic surgery (inner circle -- "Qualified Cosmetic Surgeons") as well as physicians who have not and are, therefore, not qualified to perform cosmetic surgery. Whether physicians from among the various disciplines are qualified to perform cosmetic surgery is determined by their education, training, experience, and proven competence with respect to the contemplated cosmetic procedure, and not by their underlying board certification. It is imperative that cosmetic surgery patients understand this fact. Those who only consider a physician's underlying board certification when choosing their doctor base their decision on incomplete information and reduce their choice of qualified cosmetic surgeons. See Diagram A.
Cosmetic surgery patients who believe that all board certified plastic surgeons, and only board certified plastic surgeons, are competent in cosmetic surgery may choose an unqualified physician (i.e., board certified plastic surgeon with inadequate or no training with respect to the given cosmetic procedure) and are, therefore, at risk. Compare Diagrams A and B.
Criteria for Evaluating Physicians.
The Article falsely suggests that hospitals evaluate doctors based on their board certification, and therefore patients should do the same. On the contrary, the criteria hospitals use to evaluate physicians specifically opposes relying on a doctor's board certification. Instead, the criteria for evaluating physicians applied by national healthcare organizations requires an assessment of the physician's education, training, experience, and proven competence. This criteria is consistently published by the American Medical Association ("AMA"), American Osteopathic Association's Healthcare Facilities Accreditation Program (HFAP), the Joint Commission, which accredits hospitals in the U.S., and the Federal Government. In fact, the U.S. Department of Health and Human Services expressly prohibits the granting of staff membership or hospital privileges solely on certification or membership in a specialty body or society.
Recognizing the potential abuse of specialty certification, AMA's House of Delegates adopted Substitute Resolution 88 regarding the delineation of clinical privileges:
Resolved that it is the American Medical Association policy that individual character, training, competence, experience, and judgment be the criteria for granting privileges in hospitals; and be it further resolved, that the physicians representing several specialties can and should be permitted to perform same procedures if they meet this criteria.
AMA's policy on "Board Certification and Discrimination" specifically opposes discrimination against physicians based solely on lack of ABMS or equivalent American Osteopathic Board certification. Importantly, all of these authorities agree the use of a single criterion, including board certification, in evaluating a physician is inappropriate and inconsistent with providing quality patient care.
Board Certification in Cosmetic Surgery.
Contrary to the Article's false information, there are multiple valid certifying boards that are not members of the American Board of Medical Specialties ("ABMS"), and, importantly, none of the ABMS member boards certify physicians in cosmetic surgery.
ABMS is only one of several private organizations that recognize medical specialty certifying boards that meet their membership requirements. Today, the three largest organizations that provide medical specialty board recognition include the ABMS (recognizing 24 specialty boards), the American Osteopathic Association's Bureau of Osteopathic Specialists (recognizing 18 specialty boards), and the American Board of Physician Specialties (recognizing 18 specialty boards). All three organizations assist their member boards in developing educational and professional standards to evaluate and certify physicians in their respective specialties. And, all three are private membership organizations that must consider, address, and foster the interests of their members. What a board's certification evidences about the education, training, and experience of those it certifies depends on its certification requirements; not on the membership association to which it belongs.
The American Board of Cosmetic Surgery ("ABCS") certifies physicians exclusively in cosmetic surgery. In addition to other certification requirements, all applicants for certification by ABCS must first be certified by one of the following ABMS or AOA member boards:
American Board of Dermatology;
American Board of Surgery;
American Board of Obstetrics and Gynecology;
American Board of Ophthalmology (with completion of an American Society of Ophthalmic Plastic and Reconstructive Surgery approved Oculoplastic Fellowship);
American Board of Otolaryngology;
American Board of Plastic Surgery;
or be recognized by the American Board of Oral and Maxillofacial Surgery (ABOMS) and have an MD degree. In determining certification, ABCS considers only eligible candidates who, by definition, have completed certain general surgical training and specific additional cosmetic surgery training. The residency and post-residency training required by an ABMS candidate's core board coupled with the additional training required by ABCS for certification meets or exceeds that which eligible candidates to any ABMS board (including plastic surgery) must obtain with respect to any certified cosmetic procedure. Without substantial post-residency training in cosmetic surgery, many if not most board certified plastic surgeons do not qualify for certification by ABCS.
Liposuction and the Tumescent Technique.
Importantly, the Article misrepresents facts about liposuction suggesting it is safer if performed under general anesthesia rather than local anesthesia when, in fact, the opposite is true. From the pioneering liposuction techniques introduced in Europe in the 1970s through the time it was introduced in the U.S. in the early 1980s, liposuction procedures were performed under general anesthesia. This changed in the mid-1980s when dermatologist, Jeffrey A. Klein, M.D., developed the tumescent technique. The tumescent technique, which involves local anesthesia, revolutionized liposuction and is much safer than liposuction under general anesthesia.
As confirmed in an article published in the Journal of Clinical Anesthesia (Liposuction: contemporary issues for the anesthesiologist), many physicians who perform liposuction have not made the effort to learn the new, safer procedure:
Unfortunately, many physicians and anesthesiologists, due to their limited training in tumescent anesthesia, still believe that modern general anesthesia is the safest route for liposuction. Consequently, many do not make the effort to learn the new technique that allows liposuction totally by local anesthesia. Although modern general anesthesia is considered safe, it may expose the patient to unnecessary risk given that a safer alternative is available. Now that liposuction can be performed totally by local anesthesia, it might be considered that general anesthesia is often abused in the world of cosmetic surgery. Kucera, M.D., Ian J., Liposuction: contemporary issues for the anesthesiologist. Journal of Clinical Anesthesia, 2006, 18: 380).
Most importantly, and as further confirmed by multiple fact based studies and articles over the past decade, liposuction patients of board certified plastic surgeons experienced a significantly higher death rate, insurance claims, and malpractice complaints, compared to other specialties performing cosmetic procedures.
How to Choose Your Cosmetic Surgeon.
Cosmetic surgery patients should ask their cosmetic surgeon the following:
How long have you been performing the specific cosmetic procedure?
What are the risks and possible complications? Before the surgery, your doctor should explain to you the risks and possible complications, and potential side effects, including the pros and cons of the procedure.
Where did you receive your training with respect to the procedure?
How much experience do you have performing the procedure? How many have you performed in total? How many have you performed over the past year?
How do you define success with regard to the procedure? What is your success rate performing the procedure? How many of your patients have returned for revisions or corrections with respect to the procedure? How many of your patients have returned for revisions or corrections in general?
May I review "before and after" pictures of those who have had the procedure performed by you?
Where will you perform my procedure? Is the facility accredited? Cosmetic surgery is performed in various facilities such as hospitals, surgical centers, and office settings. An accredited surgical facility must meet certain minimum standards to obtain and maintain its accreditation. Some certifying organizations include the Joint Commission (formerly "JCAHO"), the Accreditation Association for Ambulatory Health Care ("AAAHC"), and the American Association for Accreditation of Ambulatory Surgery Facilities ("AAAASF").
Are there any alternatives to the procedure that may exist considering my desired result?
The Article was based on false and misleading information. Accordingly, we respectfully urge USA Today to correct the misinformation before cosmetic surgery patients rely on the Article and are harmed.
Respectfully Submitted on behalf of:
American Academy of Cosmetic Surgery, Angelo Cuzalina, MD, DDS, President
American Board of Cosmetic Surgery, Michael Will, MD, DDS, President
Cosmetic Surgery Foundation for Education, Research and Patient Safety, Suzan Obagi, MD, President; Jane Petro, MD, FACS, Executive Director
Robert Jackson, MD, AMA House of Delegates Cosmetic Surgery Representative
1 The total number of physicians board certified in the named specialties since the Boards' inceptions (dermatology, general surgery, gynecology, ophthalmology, otolaryngology, oral and maxillofacial surgery, and plastic surgery) exceeds 176,840; with approximately the following breakdown among specialties: Dermatology: 14,330; General Surgery: 57,810; Gynecology: 49,110; Ophthalmology: 24,800; Otolaryngology: 15,960; Oral and Maxillofacial Surgery: 7,060; and Plastic Surgery: 7,770. Board certified plastic surgeons make up only 4.4% of the total number of board certified physicians shown. (ABMS 2010 Certificate Statistics; and Report of the ADA-Recognized Specialty Certifying Boards April 2011).
What Patients Should Know About Cosmetic Surgery and Their Cosmetic Surgeons
Jayne O'Donnell's articles of September 14-15, 2011 entitled "These Women died after having liposuction" and "Cosmetic surgery gets cheaper, faster, scarier: Commoditization opens door to dubious practices" (collectively "Article") jeopardize the safety of your readers considering cosmetic surgery. The Article is filled with false information, and misleads patients regarding how to choose a cosmetic surgeon placing patients at risk.
In order to protect cosmetic surgery patients who read your Article, the American Academy of Cosmetic Surgery ("AACS"), American Board of Cosmetic Surgery ("ABCS"), the Cosmetic Surgery Foundation for Education, Research and Patient Safety ("CSF"), and the cosmetic surgeons who represent the specialty of cosmetic surgery on the American Medical Association ("AMA") House of Delegates, respectfully urge USA Today to correct the false and misleading statements contained in the Article. The authors hereof, and the groups they represent, share the goal of patient safety through education. We were disturbed to learn of the tragedies subject to the Article, and it reminded us why we tirelessly advocate to ensure that only physicians who obtain the necessary education, training, and experience perform cosmetic surgery. Unfortunately, Ms. O'Donnell was misinformed, and the Article relies on anecdotal information rather than peer reviewed articles and fact based evidence.
It is our goal to provide cosmetic surgery patients with valuable and credible information regarding cosmetic surgery, and the education, training, and experience necessary to perform it. To help USA Today correct the misinformation included in the Articles, below is fact-based information regarding cosmetic surgery and who is qualified to perform it:
Plastic Surgery and Cosmetic Surgery Are Not the Same Thing.
Cosmetic surgery and plastic surgery are different specialties requiring different education, training, and experience. Cosmetic surgery involves procedures designed to enhance appearance (Common procedures include breast implants; chemical peels; chin, cheek, and nose augmentation; face lifts; hair transplants; liposuction, and tummy-tucks). Cosmetic surgery was developed, and is practiced, by dermatologists, facial plastic surgeons, general surgeons, gynecologists, oral and maxillofacial surgeons, ophthalmologists, otolaryngologists, plastic surgeons, and doctors from other fields. Unlike cosmetic surgery, plastic surgery is dedicated to reconstruction of facial and body defects due to birth disorders, trauma, burns, and disease.
There are currently no residency programs in the U.S. devoted exclusively to cosmetic surgery. And, residency programs in dermatology, general surgery, obstetrics and gynecology, oral and maxillofacial surgery, ophthalmology, otolaryngology, and plastic surgery do not include training on every cosmetic procedure. Therefore, doctors seeking to learn the vast array of cosmetic surgery procedures must do so after completing their residency training. Understanding this fact is necessary to understanding the difference between "cosmetic surgery" and "plastic surgery."
Residency training required to become board certified in plastic surgery may not include training with respect to many common cosmetic procedures. Therefore, while the title "board certified plastic surgeon" tells you the doctor has received certain training and experience with respect to "plastic surgery," it does not tell you the same thing with respect to "cosmetic surgery," and it does not tell you the doctor has more or less "cosmetic surgery" training than a board certified dermatologist, facial plastic and reconstructive surgeon, general surgeon, gynecologist, oral and maxillofacial surgeon, ophthalmologist, otolaryngologist, or other doctor. Therefore, to find the most qualified doctor for a specific cosmetic procedure, patients must compare doctors' overall (residency and post-residency) training and experience with respect to that procedure.
Cosmetic surgery patients need to understand that the education, training, and experience required for a doctor to become competent in cosmetic surgery is not the same as that required to become competent in plastic surgery. The Article's suggestion to the contrary is simply false. See Diagram A.
Diagram A
Diagram A illustrates the Article's false premises that all board certified plastic surgeons, and only board certified plastic surgeons, are qualified to perform all cosmetic procedures. Cosmetic surgery patients who believe these false premises are misled into relying on incomplete and inaccurate information when choosing their physician. As a result, patients fail to consider many well-qualified cosmetic surgeons, and fail to properly evaluate physicians' education, training, and experience regarding their cosmetic procedure. As a result, their safety is jeopardized by: (1) having their choice of qualified cosmetic surgeons arbitrarily reduced;1 and (2) potentially being directed to physicians with little or no cosmetic surgery experience.
The fact is that there are physicians in various specialties who obtain the necessary post-residency education, experience and training to become qualified to perform cosmetic surgery, and there are others who do not. Therefore, a physician's competence, skill, and ability with respect to a cosmetic surgery procedure depends on their education, training, and experience regarding that procedure, and not on their particular board certification. See Diagram B.
Diagram B

Diagram B correctly illustrates that within each discipline there are physicians who received specialized education, training, and experience in cosmetic surgery (inner circle -- "Qualified Cosmetic Surgeons") as well as physicians who have not and are, therefore, not qualified to perform cosmetic surgery. Whether physicians from among the various disciplines are qualified to perform cosmetic surgery is determined by their education, training, experience, and proven competence with respect to the contemplated cosmetic procedure, and not by their underlying board certification. It is imperative that cosmetic surgery patients understand this fact. Those who only consider a physician's underlying board certification when choosing their doctor base their decision on incomplete information and reduce their choice of qualified cosmetic surgeons. See Diagram A.
Cosmetic surgery patients who believe that all board certified plastic surgeons, and only board certified plastic surgeons, are competent in cosmetic surgery may choose an unqualified physician (i.e., board certified plastic surgeon with inadequate or no training with respect to the given cosmetic procedure) and are, therefore, at risk. Compare Diagrams A and B.
Criteria for Evaluating Physicians.
The Article falsely suggests that hospitals evaluate doctors based on their board certification, and therefore patients should do the same. On the contrary, the criteria hospitals use to evaluate physicians specifically opposes relying on a doctor's board certification. Instead, the criteria for evaluating physicians applied by national healthcare organizations requires an assessment of the physician's education, training, experience, and proven competence. This criteria is consistently published by the American Medical Association ("AMA"), American Osteopathic Association's Healthcare Facilities Accreditation Program (HFAP), the Joint Commission, which accredits hospitals in the U.S., and the Federal Government. In fact, the U.S. Department of Health and Human Services expressly prohibits the granting of staff membership or hospital privileges solely on certification or membership in a specialty body or society.
Recognizing the potential abuse of specialty certification, AMA's House of Delegates adopted Substitute Resolution 88 regarding the delineation of clinical privileges:
Resolved that it is the American Medical Association policy that individual character, training, competence, experience, and judgment be the criteria for granting privileges in hospitals; and be it further resolved, that the physicians representing several specialties can and should be permitted to perform same procedures if they meet this criteria.
AMA's policy on "Board Certification and Discrimination" specifically opposes discrimination against physicians based solely on lack of ABMS or equivalent American Osteopathic Board certification. Importantly, all of these authorities agree the use of a single criterion, including board certification, in evaluating a physician is inappropriate and inconsistent with providing quality patient care.
Board Certification in Cosmetic Surgery.
Contrary to the Article's false information, there are multiple valid certifying boards that are not members of the American Board of Medical Specialties ("ABMS"), and, importantly, none of the ABMS member boards certify physicians in cosmetic surgery.
ABMS is only one of several private organizations that recognize medical specialty certifying boards that meet their membership requirements. Today, the three largest organizations that provide medical specialty board recognition include the ABMS (recognizing 24 specialty boards), the American Osteopathic Association's Bureau of Osteopathic Specialists (recognizing 18 specialty boards), and the American Board of Physician Specialties (recognizing 18 specialty boards). All three organizations assist their member boards in developing educational and professional standards to evaluate and certify physicians in their respective specialties. And, all three are private membership organizations that must consider, address, and foster the interests of their members. What a board's certification evidences about the education, training, and experience of those it certifies depends on its certification requirements; not on the membership association to which it belongs.
The American Board of Cosmetic Surgery ("ABCS") certifies physicians exclusively in cosmetic surgery. In addition to other certification requirements, all applicants for certification by ABCS must first be certified by one of the following ABMS or AOA member boards:
American Board of Dermatology;
American Board of Surgery;
American Board of Obstetrics and Gynecology;
American Board of Ophthalmology (with completion of an American Society of Ophthalmic Plastic and Reconstructive Surgery approved Oculoplastic Fellowship);
American Board of Otolaryngology;
American Board of Plastic Surgery;
or be recognized by the American Board of Oral and Maxillofacial Surgery (ABOMS) and have an MD degree. In determining certification, ABCS considers only eligible candidates who, by definition, have completed certain general surgical training and specific additional cosmetic surgery training. The residency and post-residency training required by an ABMS candidate's core board coupled with the additional training required by ABCS for certification meets or exceeds that which eligible candidates to any ABMS board (including plastic surgery) must obtain with respect to any certified cosmetic procedure. Without substantial post-residency training in cosmetic surgery, many if not most board certified plastic surgeons do not qualify for certification by ABCS.
Liposuction and the Tumescent Technique.
Importantly, the Article misrepresents facts about liposuction suggesting it is safer if performed under general anesthesia rather than local anesthesia when, in fact, the opposite is true. From the pioneering liposuction techniques introduced in Europe in the 1970s through the time it was introduced in the U.S. in the early 1980s, liposuction procedures were performed under general anesthesia. This changed in the mid-1980s when dermatologist, Jeffrey A. Klein, M.D., developed the tumescent technique. The tumescent technique, which involves local anesthesia, revolutionized liposuction and is much safer than liposuction under general anesthesia.
As confirmed in an article published in the Journal of Clinical Anesthesia (Liposuction: contemporary issues for the anesthesiologist), many physicians who perform liposuction have not made the effort to learn the new, safer procedure:
Unfortunately, many physicians and anesthesiologists, due to their limited training in tumescent anesthesia, still believe that modern general anesthesia is the safest route for liposuction. Consequently, many do not make the effort to learn the new technique that allows liposuction totally by local anesthesia. Although modern general anesthesia is considered safe, it may expose the patient to unnecessary risk given that a safer alternative is available. Now that liposuction can be performed totally by local anesthesia, it might be considered that general anesthesia is often abused in the world of cosmetic surgery. Kucera, M.D., Ian J., Liposuction: contemporary issues for the anesthesiologist. Journal of Clinical Anesthesia, 2006, 18: 380).
Most importantly, and as further confirmed by multiple fact based studies and articles over the past decade, liposuction patients of board certified plastic surgeons experienced a significantly higher death rate, insurance claims, and malpractice complaints, compared to other specialties performing cosmetic procedures.
How to Choose Your Cosmetic Surgeon.
Cosmetic surgery patients should ask their cosmetic surgeon the following:
How long have you been performing the specific cosmetic procedure?
What are the risks and possible complications? Before the surgery, your doctor should explain to you the risks and possible complications, and potential side effects, including the pros and cons of the procedure.
Where did you receive your training with respect to the procedure?
How much experience do you have performing the procedure? How many have you performed in total? How many have you performed over the past year?
How do you define success with regard to the procedure? What is your success rate performing the procedure? How many of your patients have returned for revisions or corrections with respect to the procedure? How many of your patients have returned for revisions or corrections in general?
May I review "before and after" pictures of those who have had the procedure performed by you?
Where will you perform my procedure? Is the facility accredited? Cosmetic surgery is performed in various facilities such as hospitals, surgical centers, and office settings. An accredited surgical facility must meet certain minimum standards to obtain and maintain its accreditation. Some certifying organizations include the Joint Commission (formerly "JCAHO"), the Accreditation Association for Ambulatory Health Care ("AAAHC"), and the American Association for Accreditation of Ambulatory Surgery Facilities ("AAAASF").
Are there any alternatives to the procedure that may exist considering my desired result?
The Article was based on false and misleading information. Accordingly, we respectfully urge USA Today to correct the misinformation before cosmetic surgery patients rely on the Article and are harmed.
Respectfully Submitted on behalf of:
American Academy of Cosmetic Surgery, Angelo Cuzalina, MD, DDS, President
American Board of Cosmetic Surgery, Michael Will, MD, DDS, President
Cosmetic Surgery Foundation for Education, Research and Patient Safety, Suzan Obagi, MD, President; Jane Petro, MD, FACS, Executive Director
Robert Jackson, MD, AMA House of Delegates Cosmetic Surgery Representative
1 The total number of physicians board certified in the named specialties since the Boards' inceptions (dermatology, general surgery, gynecology, ophthalmology, otolaryngology, oral and maxillofacial surgery, and plastic surgery) exceeds 176,840; with approximately the following breakdown among specialties: Dermatology: 14,330; General Surgery: 57,810; Gynecology: 49,110; Ophthalmology: 24,800; Otolaryngology: 15,960; Oral and Maxillofacial Surgery: 7,060; and Plastic Surgery: 7,770. Board certified plastic surgeons make up only 4.4% of the total number of board certified physicians shown. (ABMS 2010 Certificate Statistics; and Report of the ADA-Recognized Specialty Certifying Boards April 2011).